Very rarely, an underlying and serious problem i.e. Hirschsprung’s disease, can be detected on biopsy.
Importantly, most biopsies done are actually negative.
However, it can be tricky moving forward with recommended treatments if there is an outstanding concern.
For parents, it can be quite difficult to decide if the time has come to discuss a biopsy with your paediatrician.
Paediatric surgeon’s are best placed to review and advise. We manage Hirschsprung’s disease and will have a good sense of whether a biopsy is needed or not.
Constipation is a common problem in childhood. Most children will have an episode that passes naturally, or with changes in diet and perhaps some medication. However, some children will have chronic, ongoing issues that escalate, needing surgical intervention.
When is a biopsy of the rectum useful?
If 10 children have a biopsy, 1 or 2 may have a positive finding of Hirschsprung’s disease.
However, a review will be necessary before the biopsy to find out if there are other risk factors.
NICE recommends that a rectal biopsy should not be performed unless there is:
-delayed meconium (>48hrs after birth in a term baby
-early constipation (first weeks of life)
-chronic abdominal distension plus vomiting
-family history of Hirschsprung’s disease
-faltering growth, in addition to any of the previous features
Suction biopsy: A small , finger-like biopsy tube is placed inside the rectum. A syringe is used to suck some of the rectal tissue into the tube, which has a cutting mechanism. A small sample is pinched off. As the sample is small, the surgeon may choose to take a 2-3 samples at different levels, to increase the chance of a clear result. Most doctors would like to do this under the age of 6 months.
This method can be carried out in an awake baby, as long as can be effectively wrapped to keep them still. Over 6 months, the baby is strong enough to move, making the test more difficult to achieve effectively.
Strip biopsy: This method involves a general anaesthetic. Once asleep, the surgeon looks inside the rectum and cuts out a 1-2cm strip of tissue.
Regardless of method, these samples are then sent to the lab.
What are the lab looking for?
In summary, nerve fibres and ganglion cells.
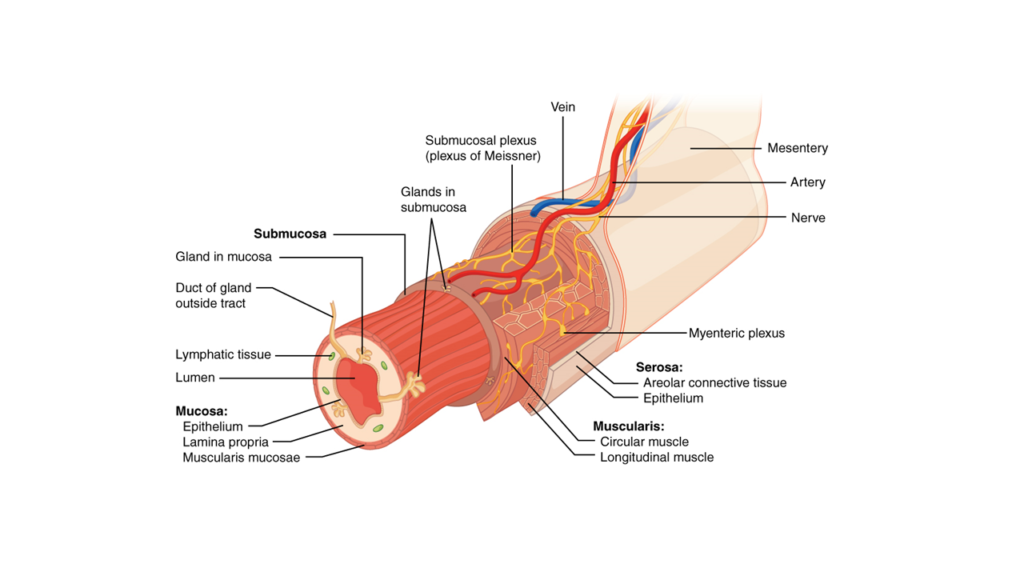
Ganglion cells are specialised hubs where nerve fibres meet and communicate. The histopathologist in the lab looks to confirm the presence of the nerve fibres and ganglion cells.
In Hirschsprung’s disease, there are no ganglion cells (hence the term- aganglionosis) within the bowel layers.
Nerve fibres are absent. Abnormally thickened nerve trunks are also observed.
This ganglion cell test is very sensitive for Hirschsprung’s disease. If the ganglion cells are seen, your surgeon can be >93% sure that your child doe not have Hirschsprung’s disease.
Dr Eva Coates is a Consultant Paediatric Surgeon at Oxford University Hospitals.
She has a sub-speciality interest, and accreditation, in Paediatric Colorectal Surgery. She has a clinical interest in minimal invasive keyhole surgery, constipation in children, anorectal malformations, Hirschsprung disease and inflammatory bowel disease.
Dr Coates completed medical training at University of Oxford and University of Cambridge. She completed higher surgical training rotations in the South East of England London and Cambridge centres. She holds a PhD from University College London, where she focused on risk stratification for children requiring fundoplication. She successfully completed the Royal College of Surgeons Senior Fellowship in Paediatric Colorectal Surgery.
Dr Coates has multiple publications and presentations covering upper and lower gastrointestinal problems affecting children. She has an ongoing interest in cohort data informatics and patient empowerment through education.
Inguinal hernia Umbilical hernia Undescended testis orchidopexy Foreskin problems, circumcision for scarred phimosis or BXO
InsurerRecognition:
AXA
Allianz
Bupa
WPA
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept All”, you consent to the use of ALL the cookies. However, you may visit "Cookie Settings" to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.