Constipation is a common problem in childhood. Most children will have an episode that passes naturally, or with changes in diet and perhaps some medication. However, some children will have chronic, ongoing issues that escalate, needing surgical intervention.
When is a biopsy of the rectum useful?
If 10 children have a biopsy, 1 or 2 may have a positive finding of Hirschsprung’s disease.
However, a review will be necessary before the biopsy to find out if there are other risk factors.
NICE recommends that a rectal biopsy should not be performed unless there is:
-delayed meconium (>48hrs after birth in a term baby
-early constipation (first weeks of life)
-chronic abdominal distension plus vomiting
-family history of Hirschsprung’s disease
-faltering growth, in addition to any of the previous features
Other features have been suggested:
–vomiting, in addition to abdominal distension is a risk factor for Hirschsprungs
-a rectal biopsy is more likely to be negative with increasing age
–girls are less likely to have a positive biopsy for Hirschsprung’s
How is the biopsy done?
Suction biopsy: A small , finger-like biopsy tube is placed inside the rectum. A syringe is used to suck some of the rectal tissue into the tube, which has a cutting mechanism. A small sample is pinched off. As the sample is small, the surgeon may choose to take a 2-3 samples at different levels, to increase the chance of a clear result. Most doctors would like to do this under the age of 6 months.
This method can be carried out in an awake baby, as long as can be effectively wrapped to keep them still. Over 6 months, the baby is strong enough to move, making the test more difficult to achieve effectively.
Strip biopsy: This method involves a general anaesthetic. Once asleep, the surgeon looks inside the rectum and cuts out a 1-2cm strip of tissue.
Regardless of method, these samples are then sent to the lab.
What are the lab looking for?
In summary, nerve fibres and ganglion cells.
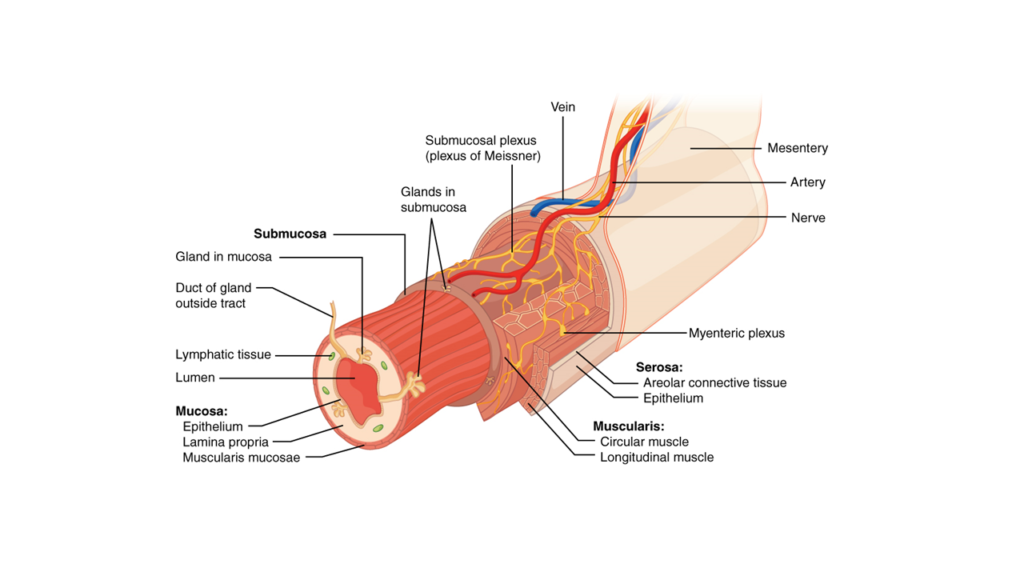
Ganglion cells are specialised hubs where nerve fibres meet and communicate. The histopathologist in the lab looks to confirm the presence of the nerve fibres and ganglion cells.
In Hirschsprung’s disease, there are no ganglion cells (hence the term- aganglionosis) within the bowel layers.
Nerve fibres are absent. Abnormally thickened nerve trunks are also observed.
This ganglion cell test is very sensitive for Hirschsprung’s disease. If the ganglion cells are seen, your surgeon can be >93% sure that your child doe not have Hirschsprung’s disease.