Circumcision referrals are a common feature in general paediatric clinics. Indeed, cicrumcision is the described as the world’s most popular surgery.
Here’s some valuable information to help filter physiological and pathological foreskins, from London Children’s Surgery.
What is the natural history of the foreskin?
This much-quoted study (Gairdner, BMJ 1949) provides a useful summary of the natural history of the foreskin.
Oster’s follow-up paper (Oster, Arch. Dis. Childh, 1968) should be read simply for its cracking opening paragraph. It also contains useful data on phimosis, preputial adhesions and smegma in Danish boys.
We expect partial or full retraction at the following frequencies:
–Birth: 4%
–Up to 6 Months: 20%
–1 year : 50%
–3-11yrs: 90%
–12-13yrs: 95%
–14+yrs: 99%
Therefore, most foreskin reviews will demonstrate physiological phimosis, and parents can be reassured.
Normal / physiological phimosis?
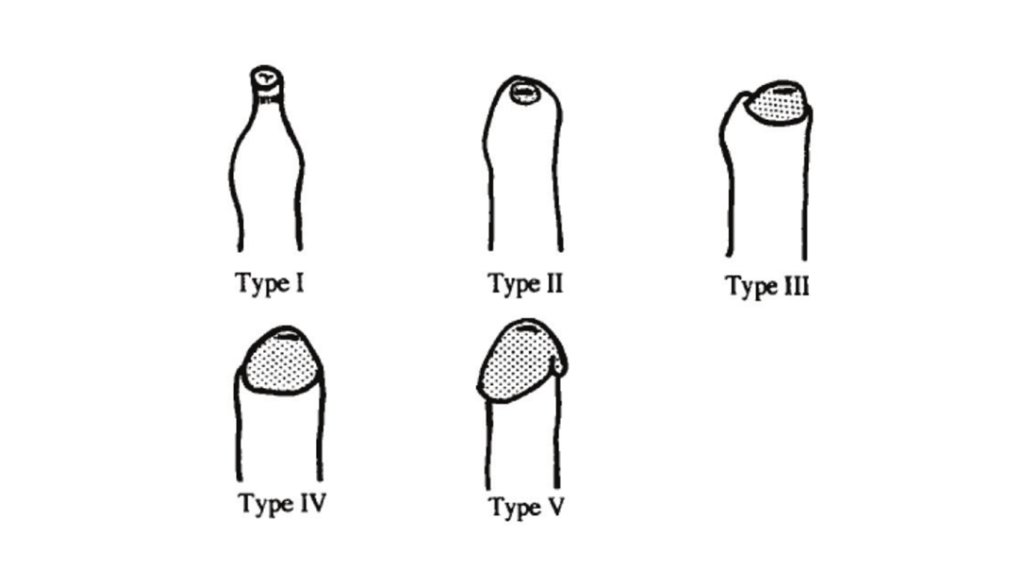
There are various classification systems for retraction of the foreskin. As described by Kayaba et al, retraction progresses from Grade I – V.
What are the features of phimosis?
Balooning
Discomfort
Balanoposthitis
Are steroids useful?
These are frequently used in primary care. The therapeutic goal is making the foreskin more supple. Steroids achieve this by suppresing fibroblast activity, causing thinning of the skin. However, they do have an anti-inflammatory and immunosuppresive effect. This limits their role to pulsed treatments.
Evidence:
-Systematic review, Moreno et al, 2014: Included 12 comparative studies (1395 boys). Compared with placebo, corticosteprids increase the probability of achieving partial or full retraction (RR2.45, 95CI1.84-3.26_
-New South Wales, Wright et al, 1994: 80% retractability achieved in 111 boys completing this betamethasone study
-Barcelona, Orsola et al, 2000: 90% of 137 boys treated with betamathosone with retraction had improvements in retractability
Betamethasone 0.05% applied twice a day over a 4-week period , is a commonly used protocol.
Other steroids favoured include hydrocortisone, clobetasol and triamcinilone.
The steroid effect may wear off, leading to a decline in retractability after a few months, necessitating a repeated course.
What about simple emollients?
Golubovic et al, 1996, found a higher frequency of inproved retraction (19/20) in boys treated with betamethasone, compared with boys treated with vaseline alone (4/20 improved).
Preputial stretching
This is described in combination with steroids , at varying frequency e.g. daily or weekly.
Importantly, any stretching should be done by the child, who will limit the stretch to what is comfortable. This will avoid secondary scarring.
What is pathological phimosis?
Pathological or True phimosis occurs when the foreskin is scarred. This is seen in :
1. Balanitis xerotica obliterans
2 Scarred balanoposthitis
Circumcision for UTI of reflux ?
UTI and VUR are described in depth elsewhere.
For the purposes of circumcision, a decision for each patient must be made. However, where surgery is proposed as prophylaxis, keep in mind the numbers needed to treat.
Number needed to treat
rUTI : 111 circumcisions to prevent 11 recurrent UTIs
VUR: 111 circumcisions to prevent 4 UTIs in boys with high grade reflux
What are the surgical options?
There are two options:
1. Dorsal slit procedure
2. Circumcision